
CUREFAQs: Frequently Asked Questions
Answers to commonly asked arterial and metabolic disease questions.
Categories
Click on one of the categories below or type a keyword into the search bar to get started.












Recent FAQs
What is Insulin Resistance? Can it be reversed?
Insulin resistance occurs when the cells of the muscles, fat, and liver become insensitive or resistant to insulin, causing the body to produce higher insulin levels to compensate…
Insulin resistance occurs when the cells of the muscles, fat, and liver become insensitive or resistant to insulin, causing the body to produce higher insulin levels to compensate in the primary goal to optimize blood glucose and its utilization as fuel. This state of hyperinsulinemia is highly inflammatory for your entire body, especially your arteries and nerves. Eventually insulin production fails and blood sugar levels begin to rise. It is at this point the patient is diagnosed with diabetes based on elevated blood glucose/”sugar”, the final stage of "diabesity."
However, even thin, lean people can be insulin resistant, especially if muscle mass is low (sarcopenia) relative to body fat, especially visceral fat.
In reality, insulin resistance is so common that we should assume its presence till proven absent. Why is it so common to be called a “feature” rather than a “bug”? Why wouldn’t evolutionary pressures get rid of it? The answer: It is a benefit to the hunter gatherer lifestyle. It is not well suited for our current cultural promotion of “grazing” constantly on sweets, starches and highly processed snacking. And, it doesn’t cause death prior to reproduction.
The answer: Eat like a hunter gatherer! Eat within a short time window (6 hours is ideal) and eat lots of vegetables, some fruit (sugary!), meat/protein and good fat (olive, coconut or avocado oil, seeds, nuts).
What is Diabesity?
Diabesity is the spectrum of adverse health effects of diabetes and obesity. It is the result of a modern environment of processed food loaded with sweets and starches consumed throughout the day.
Before rising glucose levels are detected, the higher insulin levels (caused by insulin resistance) raise blood pressure and create inflammation that contributes to arterial damage. We call this damage atherosclerosis. It can also lead to diabetes, dementia (Type 3 Diabetes?) erectile dysfunction, and depression. Risk of heart attack, stroke, and dementia also increase.
We develop "tolerance" to the toxic effects of sweets and insulin. This leads us to crave more sweets, driving our insulin levels higher, and can lead to early death and disability if unrecognized and untreated.
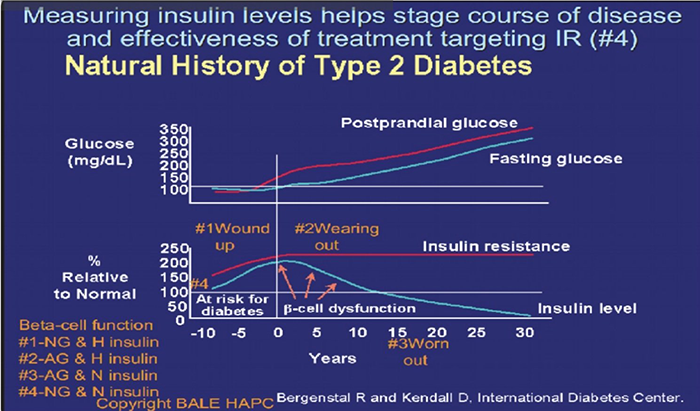
Image Source: International Diabetes Center
This graph illustrates the relationship between insulin resistance, rising insulin levels, and blood glucose levels associated with the progression from prediabetes to Type 2 Diabetes. It should be labeled "The Natural History of "Diabesity."
What are some indicators of Insulin Resistance/Diabesity?
Some indicators of insulin resistance include (but are not limited to):
Increased waist size
Elevated visceral fat
High blood pressure
Elevated blood sugar
High triglycerides
Low HDL cholesterol (Metabolic syndrome)
Small dense LDL predominance (Pattern B)
Heart attack or stroke
Gestational diabetes
Polycystic Ovary Syndrome
Erectile Dysfunction
Ananthosis Nigricans
Periodontal disease
How do we identify Insulin Resistance/Diabesity?
The gold standard identifier of insulin resistance includes a two hour oral glucose tolerance test with simultaneous insulin levels. During this test, your blood is drawn before and after drinking a sugary liquid to see how your body responds. Measuring against certain high benchmarks define diabetes and prediabetes. Normal glucose (blood sugar) levels should be below 125 after one hour of this test and 120 after two hours.
Fasting glucose levels above 90 should raise concerns about insulin resistance until other measures are used to rule it out.
Other measures used to identify insulin resistance include: high triglycerides, low high-density lipoprotein (HDL), small and dense low-density lipoprotein (LDL), hypertension, non-alcoholic fatty liver disease (NAFLD), and idiopathic neuropathy.
At the CureCenter, we perform body composition analyses on all of our patients to help identify insulin resistance/diabesity. Elevated visceral fat (which correlates with percent body fat) can be detected in a few minutes, revealing some of the earliest evidence.
Visceral fat can be hard to identify without a body composition analysis, as one may appear “thin” on the outside, but still have high levels of visceral fat. These healthy looking individuals have low muscle mass, known as sarcopenia. This occurs most commonly in women after they experience menopause, especially if they avoid resistance exercises.
How do we reverse Insulin Resistance/Diabesity?
Dietary Changes: First, cut out sweets, starches, and snacks from your diet. Excess sugar in your daily diet is stored as fat, worsening insulin resistance. Avoid sugar, artificial sweeteners, processed foods, and white bread, pasta, potatoes, and rice. These all raise insulin levels (even in the absence of high amounts of calories) and perpetuate cravings for sweets. These cravings can lead to food addiction, much like addictions to drugs and alcohol.
In order to effectively reverse insulin resistance/diabesity, be sure to eat more vegetables, protein, and good fats (from sources such as nuts, seeds, and fish).
Although fruit contains important sugar as well as vitamins, eat it in moderation. Fruit is higher in sugar (especially if dried or juiced). Eat whole fruit in limited amounts to ensure healthy glucose levels. Berries are the best. Bananas and grapes are like candy bars and M&Ms!
Exercise: Get off the couch. A sedentary lifestyle is a recipe for all types of chronic disease. While nearly all types of physical activity can be beneficial, we recommend high intensity interval training and/or a focus on building muscle through resistance training in addition to aerobic/cardio exercise.
Restricted Feeding/Fasting: At the CureCenter, we see the best results in individuals who restrict their good food intake to an 8-hour window each day. In the other 16 hours of the day, drink only water or unsweetened beverages.
For additional information about healthy fasting, we recommend resources created by Dr. Jason Fung, including his books, “The Obesity Code,” and “The Diabetes Code,” blog (The Fasting Method), and YouTube channel.
Proper Amounts of Sleep: Poor amount and quality of sleep has been linked to higher levels of insulin resistance. Be sure to get proper amounts of sleep each night. More is generally better. Very few of us get enough sleep. It is rare to get too much sleep in the absence of sleep apnea.
Manage Stress: High levels of stress have also been linked to insulin resistance. Although it’s not always easy, try to find ways to relieve stress to reduce cortisol levels that can raise glucose and insulin. Exercise is a proven and healthy way to reduce stress, so get off the couch and go outdoors or to the gym. Mindfulness practices such as meditation, prayer, or yoga can also help to manage stress.
Measure Your Results: When you first start on your journey to reverse resistance to insulin, it’s best to measure your results every 1-2 weeks by taking a body composition test (these can be done at the CureCenter office). When you’ve met your goal, continue to test every 1-2 months to ensure you are staying on track. Staying accountable is key. Seeing improvement perpetuates the process.
We call it M&M’s (the healthy kind): Measure, Motivate, and Maintain Momentum.
Supplements and Medication (if goals not achieved by lifestyle changes alone ): Sometimes, insulin resistance is so stubborn that a healthy diet and exercise do not achieve the reduction in fat that one may expect. This can be due to an incomplete commitment to carbohydrate restriction or insufficient patience. We cannot out-prescribe a bad diet. However, sometimes a little help is needed. At the CureCenter, we will prescribe medications and/or supplements that best suit your needs and lifestyle.
I’m often asked about metformin. Metformin reduces glucose primarily by reducing release of glucose from liver stores of glycogen, but it is also considered an insulin sensitizer. There is a lot of interest in it as an antiaging and anticancer treatment. Its impact on cardiovascular outcomes is not as impressive as pioglitazone, a thiazolidinedione medication.
Pioglitazone improves insulin sensitivity. It is generic and has been around for a long time. It suffers from a bad reputation for fluid retention because its use was delayed till patients with Type 2 Diabetes had failed 1st line drugs that increased the risk of heart damage from prior heart attacks. But when used in the prediabetes stage, before the damage to the heart, it is well tolerated and dramatically reduces the risk of heart attack (>70% reduction) while lowering insulin levels. See Figure 3:

What is a Carotid Intima Media Thickness (CIMT) Ultrasound?
As part of your CurePlan, you will likely be asked to get a Carotid Intima Media Thickness (CIMT) ultrasound. This is different from the ultrasound done during our CureScreen process or the ultrasound you can get at your hospital or vascular specialist…
As part of your CurePlan, you will be urged to get a Carotid Intima Media Thickness (CIMT) ultrasound if possible. This is more detailed than the CureScreen carotid ultrasound process, carotid duplex ultrasound you can get at your hospital or vascular specialist or Lifeline Screening. It provides a much more detailed look at your artery wall and measures arterial inflammation, which is the measurable and reversible underlying condition of interest.
Lifeline screening identifies and encourages “monitoring” of plaque, but does not report intima media thickness for monitoring or offer a plan other than referral for surgery for late stage disease. It is useful for screening but not monitoring or proactive early intervention. If you have had a CureScreen ultrasound, you already have more information then a Lifeline Screening ultrasound will offer, making it a waste of time and money better spent on a Carotid Intima Media Thickness ultrasound for disease monitoring.
CIMT measures the thickness/inflammation of the artery wall and characteristics of plaque using ultrasound. It is typically repeated every 6-12 months saving images and measuring the artery wall thickness. Specifically trained providers with Butterfly ultrasound probes can provide images sufficient for CIMT reports.
A thicker wall is a sicker more inflamed wall with a higher risk of developing new unstable plaque. This inflammation triggered by injury and oxidative stress from many sources sets the stage for plaque development and rupture, the event leading to stroke, heart attack, dementia, erectile dysfunction, kidney failure, or other serious complications.
Having a little bit of arterial disease is like having a little bit of cancer. Like early cancer detection, our goal is to reverse arterial disease and achieve durable remission. When cancer remission is prolonged and stable, we think of it as cured. CIMT offers the most cost-effective, painless way to monitor progress toward a cure for arterial disease.
What is the difference between a CIMT and a duplex carotid ultrasound?
The CIMT offers more meaningful information about early arterial disease than standard duplex carotid ultrasound. It documents the type of plaque (estimating risk of rupture) and measures the thickness/inflammation of the artery wall.
The purpose of the duplex carotid ultrasound is to support the need for a surgical procedure by detecting late-stage disease while watching reversible early disease progress. Additionally, if you get a duplex ultrasound, your insurance likely won’t pay for the more informative CIMT exam for at least six months. Many vascular labs mistakenly or misleadingly answer “yes” when asked if their ultrasound is a CIMT. The best bet is to go with one of the 2 providers nationwide that offer reliable and consistent CIMT testing at locations and times around the country: Vasolabs and Cardiorisk.
At the CureCenter, we depend upon the CIMT because it allows us to detect reversible early disease, assign an “arterial age,” and show your improvement – something the duplex carotid ultrasound doesn’t do. This added information and ability to track your progress will motivate your journey to optimize your CurePlan and rid yourself of chronic disease.
A new process enables measurement of CIMT based on scans obtained by medical,dental and other professionals using point of care ultrasound supported by CureCoach, the Butterfly iQ ultrasound device and Vasolabs. Ask your dentist or doctor to consider this lifesaving opportunity for addition to their skill set and services.
What is arterial age?
The health of your carotid arteries reflects the health of arteries throughout your body - including the coronary arteries that supply blood to the heart. The carotid arteries are an accessible sample of a massive supply system.
Thickness of your artery wall is compared to other people your age and gender as a population percentile. Your “arterial age” is the age for which the thickness of your arteries would be average, i.e. 50th percentile. At the CureCenter, we monitor arterial age every 6-12 months to ensure our plan is working and your arterial age is improving. If it is not improving, we look for additional opportunities to improve your CurePlan.
Does Insurance Cover CIMT?
Medicare and most insurance covers CIMT if arterial disease is present, flow velocity measurements are included and performed by a certified sonographer. This limits the number of providers who can offer this covered version. Cash payment options make it affordable for those with high deductibles or coverage only for catastrophic care.
Recently, it has become possible to provide equivalent relevant information using Butterfly point of care ultrasound in the hands of doctors, dentists, and others. This makes it more available at more times in more places. The process is not payable by Medicare or insurance coverage because it doesn’t meet their criteria. It is more than sufficient to detect disease and measure regression/improvement. The cost is $198, making it an affordable out of pocket expense compared to the cost of disability and death.
Get Started on the Path to a Long and Healthy Life

Participate in a 15-30 minute Zoom or phone call with Dr. Backs. Your questions about process, cost, insurance coverage and expectations will be answered. You will decide together if the CureCenter and a CurePlan are right for you.

Located in Central Illinois? Schedule your 15-minute CureScreen for arterial disease. It’s quick, painless, and is the first step toward preventing the most common cause of death and disability.